Blunt Thoracic Trauma
Blunt Thoracic Trauma-Analgesia Guideline
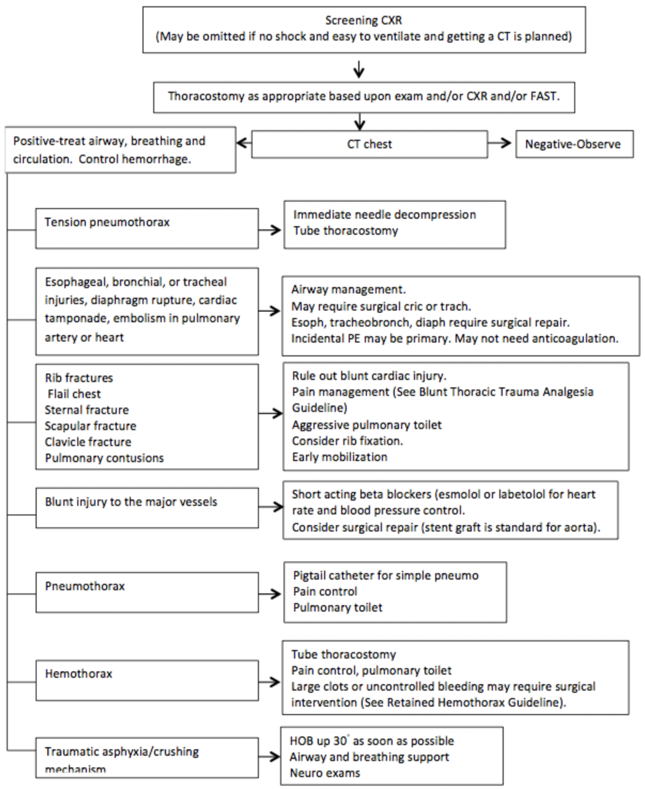
Blunt thoracic trauma (BTT) is a significant cause of morbidity and mortality. BTT is comprised of many injuries including but not limited to; rib fractures, pulmonary contusion, sternal fractures, pneumothorax, hemothorax, flail chest and soft tissue injury.
The most common injury we manage in BTT is rib fracture. Morbidity and mortality increases as the number of rib fractures increase. Associated pulmonary compromise occurs with rib fractures, including pulmonary insufficiency that can lead to respiratory failure. Pulmonary complications occur in up to one-third of BTT patients and pneumonia in 30% of cases[1-3].
Mortality is indirectly related to the rib fracture(s) but more directly a result of the respiratory embarrassment that can lead to pneumonia and/or requirement for mechanical ventilation[3-5]and this effect is more pronounced in those aged ≥ 65 [1, 6-8].
Treatment for BTT varies upon the patient, type of injury and experience/resources of the center. Typically rib fractures without significant displacement and/or restriction of the thoracic cage are treated with aggressive pulmonary toilet and pain control. The type of analgesia regimen is dependent upon many variables, including age, number of rib fractures, degree of pulmonary insufficiency and concomitant injuries. The Eastern Association for the Surgery of Trauma (EAST.org) has a practice management guideline based on an exhaustive review of the literature. Their recommendations are as follows for BTT, published in the Journal of Trauma, 59(5):1256-1267, November 2005
At VBMC, patients that have significant pain symptoms should be considered for VATs and cryoablation for pain control.


Level 1
1. Epidural
analgesia is the optimal modality of pain relief for blunt chest wall injury
and is the preferred technique after severe blunt thoracic trauma.
Level II
1. Patients
with 4 or more rib fractures who are>65 years of age should be provided with
epidural analgesia unless this treatment is contraindicated.
2. Younger
patients with 4 or more rib fractures or patients aged>65 with lesser
injuries should also be considered for epidural analgesia.
Level III
1. The
approach for pain management in BCT requires individualization for each
patient. Clinical performance measures (pain scale, pulmonary exam / function,
ABG) should be measured as judged appropriate at regular intervals.
2. Presence
in elderly patients of cardiopulmonary disease or diabetes should provide
additional impetus for epidural analgesia as these comorbidities may increase
mortality once respiratory complications have occurred.
3. Intravenous
narcotics, by divided doses or demand modalities may be used as initial
management for lower risk patients presenting with stable and adequate
pulmonary performance as long as the desired clinical response is achieved.
Mechanical stabilization
of rib fractures is reserved for those patients with severe BTT and flail
segments. Open reduction and internal fixation (ORIF) depends
largely on the degree of chest deformity and pulmonary embarrassment. Patients
must have aggressive pain control, often with epidural or paravertebral
analgesia. If these patients still have poor pulmonary reserve or
pending respiratory failure they should be considered for ORIF of the thoracic
cage and sternum as indicated, see our algorithm for chest wall fixation.
NOTE ON FOLEY’S-Thoracic epidurals do
not specifically require Foley catheterization. If criteria for discontinuation
are otherwise met, the Foley should be removed. If urinary retention occurs,
replace the Foley.


References:
1. Ziegler AW, Agarwal NN: Morbidity and Mortality of Rib Fractures. J
Trauma. 1994;37:975-979
2. Bolliger CT, Van Eeden SF. Treatment of multiple rib fracture: randomized
controlled trial comparing ventilatory with nonventilatory management Chest 1990;97:943-948
3. Bulger EM, Arneson MA, Mock CN, Jurkovich GJ. Rib fractures in the
elderly. J Trauma . 2000;48:1040-1047
4. Barnea Y, Kashtan H, Shornick Y, Werbin N. Isolated rib fractures in
elderly patients: morality and morbidity. Can J Surg. 2002;45:43-46
5. Clark GC, Schecter WP, Trunkey DD. Variables affecting outcome in blunt
chest trauma: Flail chest vs pulmonary contusion. J Trauma. 1988;28:298-304
6. Svennevig JL, Bugge-Asperheim B, Geiran OR, et al. Prognostic factors in
blunt chest trauma: analysis of 652 cases. Ann Chir Gynaecol. 1986;75:8-14
7. Shorr RM, Rodriguez A, Indeck MC, Crittenden MD, Hartunian S, Cowley RA.
Blunt chest trauma in the elderly. J Trauma 1989;29: 234-237
8. Cameron P, Dziukas L, Hadj A, Clark P, Hooper S. rib fractures in major
trauma Aust N Z J Surg. 1996;66:530-534